
26 May Pain Behind Knee: The ‘Ol Wallet-In-Door Syndrome
Author’s Gratitude: Big thanks to Dr. Ed House at New York Chiropractic College for sticking his wallet in the door during every Active Rehab meeting. The vision of him, not saying a word, and doing this, has forever been engrained in my mind.
—
Do you have pain behind knee? (That’s how they said it back in the days when the Native Americans ran around this land.)
You probably have the ‘Ol Wallet-In-Door Syndrome.
“Pain” Behind Knee Is Most Commonly Not A “Problem” Behind Knee
Test yourself.
Stand up.
Keep your knees straight and touch your toes.

If doing this provokes pain behind your knee, you have a sciatic nerve problem, either coming from an entrapment along the sciatic nerve’s course or from the spine.
This post is not about sciatic nerve “pain behind knee”. That’s for another time.
Now, sit down.
Bend your knee, bringing your heel as close as you can to your butt cheek. If it’s really painful, you can use your handy dandy friend to help you perform this test. Notice in the below example, her knee flexion range of motion stops with her heel 4 finger-breadths away from her butt cheek.

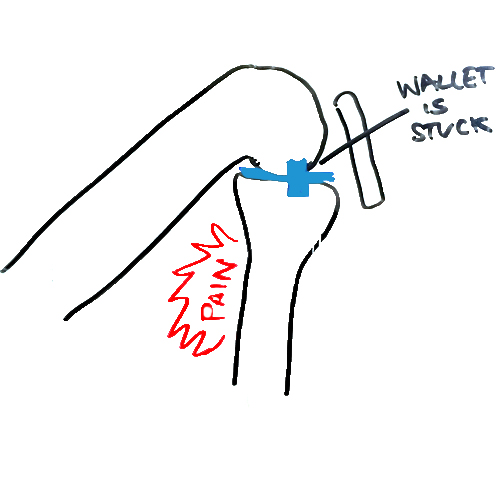
If doing this provokes pain behind your knee, you have a wallet-stuck-in-your-knee-door.
Let me explain.
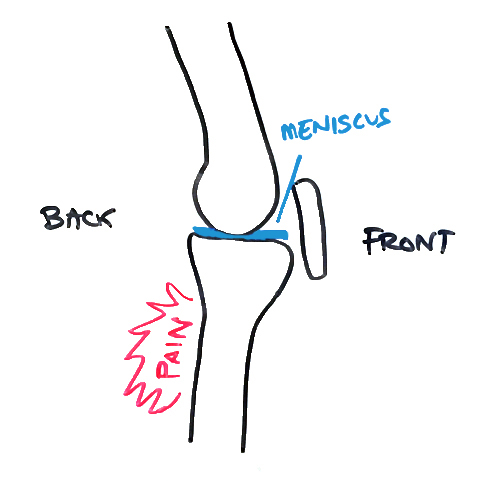
The wallet is medically speaking, a space-occupying-lesion. It is something that takes up space in the door hinge, not allowing it to fully close.
Most often, the wallet is a meniscus pathology, but it could also be osteoarthritis.
What is causing the wallet in the knee door hinge?
As always in reducing pain and restoring range of motion, we have to determine a diagnosis (a name for which problem this is).
You know if your “wallet is stuck” when:
- PAIN: you have pain behind the knee.
- FLEXIBILITY: you cannot bring your heel to your butt (you have restricted knee flexion range of motion).
In the case of the wallet in the knee door hinge, below is a simplified version of the two major issues:
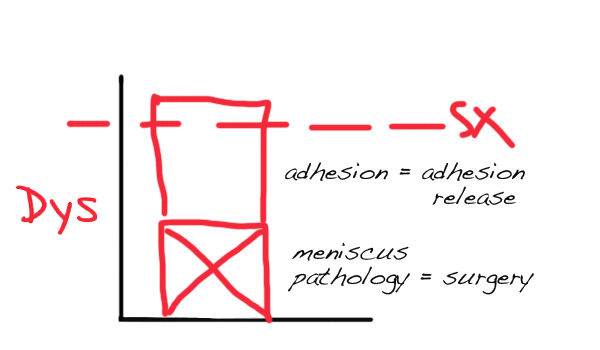
The more significant and more reducible block on our graph is the adhesion.
Removing the adhesion will slow the meniscus pathology’s growth over time.
If the meniscus pathology expresses its symptoms:
… then it may need to be reduced with surgery.
Note: Surgery, in this humble doctor’s experience, never completely resolves meniscus issues. It only makes the block smaller, it doesn’t disappear it.
How do you fix this knee problem?
The first place to look for knee adhesion by a practitioner is addressing knee flexion range of motion.
Knee flexion will be restricted, causing pain behind the knee, and creating an excessive amount of tension that can be felt by a skilled practitioner in the:
- knee capsule.
- patellar tendon.
- where the anterior, medial, and lateral meniscus touches the capsule.
- between the LCL and MCL ligaments and the capsule.
This adhesion is present due to overload of the front of the knee. This happened due to ankle and hip restriction and weakness.
Treatment to remove adhesion in the above named structures immediately increases the range of motion and causes permanent, sustainable improvement, even without further treatment.
If the pain goes away temporarily, then comes back, the meniscus pathology (and potential acute inflammation in the joint) is larger than desired. : (
After knee flexion range of motion plateaus in its improvement, adhesion should be explored in the hip and ankles to restore those ranges of motion and increase strength.
 Tell us about your pain behind the knee? Who have you seen? Did it work? How long have you had this problem?
Tell us about your pain behind the knee? Who have you seen? Did it work? How long have you had this problem?
—
If you know of a friend or family member with pain behind knee or restricted knee range of motion, please forward this information to them so they can get the help they need. Fixing your adhesion matters because it improves flexibility, improves function, reduces pain, and restores normal movement to the body so you can enjoy the things you love. Call us at 862.205.4847.

Know Your Numbers: The Face-Up Heel to Butt Test
Posted at 19:49h, 18 June[…] ability to differentiate a knee joint problem (the ‘ol wallet in the door syndrome) from a quadriceps muscle problem can save the knee from imminent […]
John Peterson
Posted at 11:36h, 08 JulyThe knee joint is the most prone joint due to the fact that of its complicated structure and also commonly worry on it. Find out more concerning the causes as well as additional treatment at this resource https://nydnrehab.com/what-we-treat/knee-pain/. It explains full photo of the illness.
Dr. Chris
Posted at 16:00h, 09 JulyThanks for your comment John.
Lara Castanha
Posted at 21:13h, 21 AugustI am having pain on the left side and behind the left knee for more than a month. It makes me immovable suddenly. . Which Physiotherapy Center or medication can help me in Alameda or Oakland CA.
Dr. Chris
Posted at 10:46h, 22 AugustHi Lara,
First, with pain behind the knee, you almost definitely need an MRI. Have you had one? You have structural damage and it will be important for the treating doctor to know how much progress they can expect with you.
I’d see this PT: http://www.solpt.com/
They should be performing Graston on your knee capsule to improve your heel to butt ROM. You should notice improvement between 1-5 visits. If you don’t see and feel progress, it'[ll be time to find a different doctor.
Here for you.
V Walsh
Posted at 18:29h, 11 MarchHi! I have this exact pain and reduced joint movementin my right knee but my doctor is very disinclined to believe I have any issues with my meniscus and is even more disinclined to refer for an MRI! I have no pain when running, swimming or cycling just when kneeling on the floor and stiffness after a long drive (no swelling). When I tore my acetabular cartilage the docs were surprised they could not the induce pain they would normally expect when they finally scanned my hip and saw a large tear. I am mildly hypermobile, do you think this could explain the increased flexion with no pain? I am training to be a midwife and being able to kneel is imperative! Whilst I understand it is hard to comment without physical assessment I would be grateful for comment. Thanks.
Dr. Chris
Posted at 11:01h, 12 AprilIf your doctor doesn’t give you an MRI, find a new doctor who does.
Sean Spraggett
Posted at 15:44h, 15 FebruaryThe first bit of information that I have read which seems to explain my behind the knee pain. I had full rupture of my left achilles and had PARS surgery (Dec 8 2019). Nine weeks later I am walking in shoes, exercising and doing PT. However, I always have this numb pain behind my knee and tight hamstring. Did your test and I am four fingers. Was wondering what I can do to help alleviate the pain and get rid of it as it is disrupting my sleep significantly.
Dr. Chris
Posted at 13:11h, 19 FebruaryHi Sean, the PARS surgery doesn’t explain the numb behind the knee and tight hamstring. However “sciatica” from the external rotators or low back does explain the overloaded achilles. Also sound like you have a knee problem, which is likely secondary to “sciatica”.
I wouldn’t be able to offer you anything for relief except to find an adhesion removal specialist. It sounds like there is a lot of stuff going on. Anything you tried would be a diminishing return or temporary relief. LMK thoughts.
Roxy Bee
Posted at 01:34h, 02 NovemberHey Dr. Chris, thank you so much for this post. Lol Though I don’t think I would have liked to hear the name while having the test performed, I’m glad to know this is worth being seen for. I have RA, hyper mobile (but pretty steady) joints and I’m used to overuse strain. The decrease in the range of motion in my knee is unsettling. However, being immunocompromised in a pandemic, I was worrying a lot about being seen unnecessarily. If you hadn’t written and published this, I may have put it off for another month or two. Thank you.
Dr. Chris
Posted at 21:59h, 02 NovemberTY for kind words Roxy. I get it. If you aren’t eating an anti-inflammatory diet, sleeping 8 hours a night, and managing stress, that will help significantly with the RA. That’s a cureable disease!
If we can help you with that process, feel free to reach out. <3
Megs
Posted at 09:47h, 23 DecemberHello Dr Chris,
I have had severe left knee pain for a year without a diagnosis yet. The pain is not in my knee as such, but on the left lateral side of the leg/knee; sometimes it is on the medial side of the knee, and sometimes it is in the lumpy boney bit on the lateral side just underneath the knee, where the bone is. As I walk, it becomes so painful that I am unable to walk. I now have crutches and often cannot go to work, shopping or live a normal life. I might have one or two days where I can walk very slowly, resting often, and get around, but it comes and goes.
I had two episodes of severe knee pain in 2019, that had me immobile and in excrutiating pain for about 1-2 weeks. The pain suddenly disappeared, and I was back to my normal life, exercising and running.
In January 2020, severe pain came on again and never left.
Two orthopaedic surgeons have assessed my knee and said there is no injury. I have had 1 Xray, 2 ultrasounds, 1 knee MRI, a lower body MRI, a full body CT scan and numerous blood tests, I also had a spine xray and was told it was fine. My doctor thinks my aenemia is causing the pain, and recommended I eat a green apple a day. Another doctor has said I now have mild sacroilliac joint disease from not being able to walk properly for so long.
I am able to perform gentle exercises (not any variants of squats or lunges) without pain, however my left groin is very tight and painful when moving my leg away from my midline now, too.
I am an otherwise healthy and used to be active person, struggling every day trying to work out what is wrong with my leg.
I would love your advice. Thank you in advance for reading this, and for your time.
Dr. Chris
Posted at 13:19h, 23 DecemberHi Megs, sorry to hear this. If you have anemia – an apple won’t help. You need meat – it’s the most bioavailable form of iron assuming you have no other metabolic issues getting in way of absorbing iron.
Yeah, sounds like you have a lower lumbar disc problem (Get a lumbar MRI) that is compromising tight groin, causing hams to go weak, which is overloading the knee. Hard to say without an exam though.
If you can find an adhesion specialist near you to unload the low back (SI Joint), sciatic nerve and knee – I highly recommend it: https://integrativediagnosis.com/find-an-id-provider/
megs
Posted at 21:41h, 23 DecemberThank you so much Chris!
Dr. Chris
Posted at 13:00h, 25 December<3
anna
Posted at 10:33h, 30 MayHi Dr. Chris,
Wow i just read all of the comments and your replies and i love how knowledgeable you are about the symptoms from different body parts being connected! (Could you please explain that to UCLA lol)
Ok so: I have had pain and swelling behind my left knee since February (3 months) not cyst, swelling is too diffuse. Nerve pain (like random electric shocks (varying intensities) by knee and also in big toe, in addition to peroneal by knee and just random nerve pain in left leg, in hip sometimes too — but doesn’t really feel like what i know of sciatica – which I’m pretty sure i have on the other (right) leg and pelvic/groin area.
I’ve had problems with my low back for like my entire life, but i always thought i just pushed it too hard when i worked out etc, but lately I’m really starting to think i could have a bulging L4/L5 or something. Often (maybe every time lately?) my lower back/tailbone area goes numb when i sit for longer than like an hour. Do you think a bulging lumbar disc could be causing the pain/swelling in my popliteal region and maybe i do have sciatica on the left side as well, its just presenting differently?
Just to add in case you see any correlations, but I also have peroneal tendonitis on right side really flaring up lately (injury from 2017) that started going into my knee cap and I’m now wearing an ankle brace for which is really helping, as well as more sciatica like symptoms on that side.
I should add, I’m 30, super healthy, worked out 5 days a week (up until quarantine). I would work out now but some days i can barely move. Also when i do my at home PT exercises (like supine hamstring stretch), i feel pins and needles in my feet/shin and when I’m done with upper and lower exercises i get random little (nothing too intense but still weird) electric shocks all over my body… i probably get them in the office too and even before when i was super active but i just don’t pay attention… I also have mildly bulging discs in neck (c4/c5 and c5/c6 and TOS left side so those could explain most of upper body stuff but not lower body…
sorry that’s a lot! it’s just all acting up at once so kinda borderline desperate over here 🙁
Thanks so much 🙂
Dr. Chris
Posted at 19:06h, 30 MayTY for kind words Anna. Have you heard of double/triple crush? Sounds like you have multiple nerve entrapments. Yes, I’d say low back is definitely primary since you have several peripheral nerves. Then it’s just a matter of removing adhesion around all of the discs in low back and nerves in leg. If you haven’t already, I’d stop pushing through pain. It will likely cause this to get much worse in next few years if you don’t listen to what your body is trying to say to you.
Dr. Chris
Posted at 10:02h, 16 JuneTY for kind words Anna.
The disc and nerve are related but not the direct cause of posterior knee symptoms. We need a “pain generator” there, or a tissue responsible for the swelling behind the knee. A compromised sciatic nerve wouldn’t inflame the tissue like that locally.
All good my friend.
If you want, you can call the office to schedule a virtual consult with me. Even if you would never come to the office, people are often happy with the diagnostic info I can give them to point them in the right direction.
anna
Posted at 05:18h, 04 JuneHi! No, i have not heard of it but i just did a basic research and i think that totally makes sense and resonates. I just found some really interesting stuff i bookmarked to read/watch — thank you so much! I actually just met another woman in my pool therapy today who has the exact same symptoms, exact same limbs/sides — so crazy God put us together. I am going to do some research and then tell her all about it too. Thank you so much again, I wish you were on this coast so i could work with you. No, i don’t push thru pain anymore, but i should have listened to my body much sooner ;( If I find out you were right, i will def let you know 🙂 God bless <3
Dr. Chris
Posted at 10:03h, 16 JuneAll good friend. If it’s ever bad enough, pls fly to us. We just had a woman fly from Texas. She was very happy she did. 70% better even after a month has gone by. : )