

09 Apr Know Your Numbers: The Thigh to Chest Test
The King Daddy of hip mobility tests is the thigh to chest test. It’s the best. ~Barefoot Rehab
So … your hips are bothering you, hey?
Don’t make me go Canadian on you. (Did you know Dr. Curtis is Canadian? Watch his perfect Canadian hair in the 2 minute video below.)
If you don’t know your hip flexion range of motion, you’re reading the right post.
The hip joint is arguably the most important joint to be concerned about.
The hip should have the strongest muscles in the body surrounding it. Nobody ever wrote a song about a small butt and the hamstrings are the primary stabilizer of the knee. When those muscles aren’t clear of adhesion and strong, it’s only a matter of time before the low back, knees, and ankles take a beating.
The most important test to determine hip integrity is supine hip flexion or the thigh to chest test.
We will measure hip flexion before extension, external rotation, internal rotation, abduction, and adduction because the most functional movement for Homo sapiens concerning the hip is flexion. Think of hip flexion any time you are sitting, whether on a chair or on the toilet bowl.
Because we Homo sapiens tend to lose range of motion when we hold sustained postures without allowing new blood to clean up the area of debris and garbage (aka free radicals), checking the range that we need to be able to sit and not load the low back becomes of paramount importance.
Disclaimer of Peace for Therapist and Fitness Coaches
If you work with clients and their ranges of motion in any capacity, you may be upset at what I’m about to say.
There are only two structures that limit this range of motion.
The structures that limit the thigh to chest test are:
- Posterior hip capsule
- Adductor magnus
Notice what is not on the list.
- Hamstrings
- Glutes
- Hip external rotators
The above data comes from the Integrative Diagnosis diagnostic system and the test-treat-retest method of developing musculoskeletal expert intuition.
Feel free to test the tissue above yourself. I did, and have found restricted hip flexion to be caused by the above tissue. Or, when range of motion does not improve, structural dysfunction such as disc or hip space-occupying-lesion, is present.
Judge for yourself.
Mobility: Thigh to Chest Test | Supine Hip Flexion (SHF)
The ability to easily bring one’s thigh to the ribs is something that anyone should be able to do, when healthy. The “Thigh to Chest Test”, or in mechanical terms, supine hip flexion, will let us know if you have that ability.
What do I need to Measure this Test? You will need a place to lie on your back and a partner to help you measure this test.
You can not do this alone because you want to test this range of motion passively (without your own muscles moving the joint). Doing so will give you clearer picture of the integrity of the joint than if you were do the test actively (with your own muscles).
What is the Thigh to Chest Test assessing? The mobility of your hip joint integrity. These structures include bone, ligaments, tendons, cartilage, and muscles.
What Specific Dysfunctions are relevant here? Besides adhesion of the two structures that limit hip flexion, there are a wide range of hip and lumbar pathologies that can permanently limit the range. The primary suspects are hip osteoarthritis, CAM/Pincer malformations of the hip, lumbar disc pathologies that take up space outside of the spinal canal (and thus limit hip range of motion), etc.
What You Need to Know: The most common symptom present during SHF will be a “pinch” sensation in the front of the hip joint. This is an impingement that usually combines soft tissue and bony pathologies.
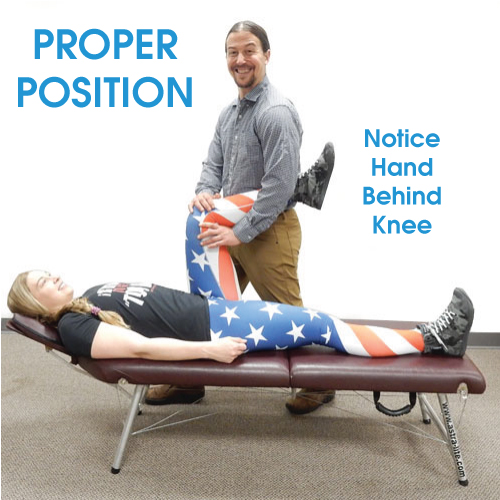
How to Test: Have your friend stand with your hand behind your thigh. Their instruction should be to bring their thigh straight up towards your armpit. In some cases, your leg might want to move away from the midline of your body. Do not let this happen.
Dr. Curtis demonstrates the thigh to chest test in the 2 minute video below.
Write this number down. Any mobilization, stretching, or treatment interventions are attempts to increase this number. If the number isn’t increased after a month, you’re wasting your time.
PASS:
A pass for this test is the ability to touch your lowest ribs with your thigh (best visualized from the side). Be sure that the thigh comes straight up towards the ribs from the lying position. The thigh might want to come away from the midline of the body. Do not let this happen.
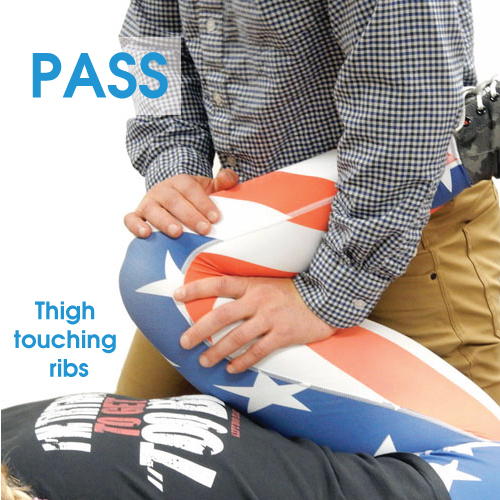
- Range: thigh touches the lowest ribs.
- Effort: Fast and easy.
- Symptoms: No symptoms. No symptoms includes the feeling of a stretch. Ideally, there would be no stretch.
FAIL – LOW RISK:
A fail is any range between touching the lowest ribs and 2 finger-breadths away.

- Range: Between touching the lowest ribs and 2 finger-breadths away.
- Effort: Fast and easy.
- Symptoms: You may feel a pinch in the front of the hip (indicating an “impingement”) or a stretch/pain in the groin (indicating likely “adhesion” in the adductor magnus) or hamstring (indicating “adhesion” in the posterior adductor magnus or referral symptoms from the hip or low back).
FAIL – HIGH RISK:
A fail, with an individual having no business doing any non-essential squatting exercises, is any range where the thigh is more than 2 finger-breadths away from touching the lowest ribs.

- Range: More than 2 finger-breadths away from touching the lowest ribs.
- Effort: May be slow, labored, and your partner might feel your hamstring contract to avoid the motion.
- Symptoms: You may feel a pinch in the front of the hip (indicating an “impingement”) or a stretch/pain in the groin (indicating likely “adhesion” in the adductor magnus) or hamstring (indicating “adhesion” in the posterior adductor magnus or referral symptoms from the hip or low back).
Movement Faults
The right away for your assisting doctor to perform this test is to bring the thigh straight up to the chest.

The primary movement fault is when the assisting doctor allows the hip to move away from the midline of your body (or abduct) as the thigh comes toward your chest.

Another movement fault that occurs is when the thigh that is resting on the table starts to magically rise off the table as your assisting doctor pushes the opposite thigh. This is a compensation. Your range of motion number stops when that opposite thigh starts lifting. Do not let the doctor push through it to come up with an artificial number.
Your hip will regret those lies.


I Know My Numbers – What do I do now?
Insanity: doing the same thing over and over again and expecting different results. ~Albert Einstein
There are a plethora of mobility and stretching resources out in the interweb for you to experiment with. It is not our intention to give prescriptive answers, simply to bring awareness to where your body currently is in time.
Use whatever tools you’d like to use for a month, stretching about ten minutes a day, for three days a week, for a month.
After a month, re-test.
If you’ve gained range of motion, wonderful! Wash, rinse, repeat, and continue stretching.
If you’re no more flexible or mobile than you were before, STOP THE INSANITY AND THE STRETCHING! It’s now time to see a Manual Adhesion Provider or Active Release Technique Provider to diagnose your condition and potentially remove the adhesion in relevant tissue to restore your mobility before you go on layering strength on top of unhealthy tissue.

While you’re awaiting 30 days from now to reassess, you might as well get baseline measurements for your ankles and your low back.
 What are your thigh to chest test numbers? Please share range, effort, and symptoms below and we can discuss what you should be doing to restore musculoskeletal integrity.
What are your thigh to chest test numbers? Please share range, effort, and symptoms below and we can discuss what you should be doing to restore musculoskeletal integrity.
—
If you know of a friend or family member with hip pain or a restricted thigh to chest test, please forward this information to them so they can get the help they need. Fixing your adhesion matters because it improves flexibility (and allows you to pass this test), improves function, reduces pain, and restores normal movement to the body so you can enjoy the things you love. Call us at 862.205.4847.

Know Your Numbers: The Thigh to Chest Test | Primal Docs
Posted at 12:01h, 10 April[…] Know Your Numbers: The Thigh to Chest Test […]
Know Your Numbers: The Lunge Stretch Test
Posted at 19:26h, 16 April[…] awaiting 30 days from now to reassess, you might as well get baseline measurements for your hip flexion, ankles and your low […]
Case Study: Hip Joint Pain in a 30 year old Female Weightlifter
Posted at 16:49h, 09 June[…] Thigh to Chest Test – takes 2 minutes to test yourself. You’ll need a partner and somewhere to lie down. […]
Alexander Zecos
Posted at 10:33h, 15 AprilHello Dr. Chris,
I believe I have agitated my right glute max along its origin points from the gluteal line of the illium, aponeurosis of the erector spine, all the way down the posterior sacrum and coccyx to the ishium. I can feel my sacrotuberous ligament where the glute max inserts into the ishium is highly agitated by palpating it. My right ishium/sitz bone always hurts when I sit down on it, and I feel a very uncomfortable stretch all along those aforementioned origin points while doing this knee to chest test. Another test I fail at even harder is when I lie face down on my stomach, bend my knee 90 degrees, and then try to kick up to the ceiling my thigh barley even gets off the floor due to this glute pain. This agitation in my glute max rarely aches or sends any signals of pain when I’m relaxed laying in bed, and it doesn’t bother me too much while walking around. Only when I’m standing for prolonged periods of time my glute max seems to struggle too much and keeps failing to keep my hips stable. And like I already mentioned sitting on my sitz bone is always too umcomfortable to bare so I have to lean to the left.
Could you describe to me any manual adhesion release techniques to cure this type of hip pain please? I’ve had this problem for 3 months now and my body has had a lot a time to try and heal on its own. I’ve been to several massage therapy sessions and one physical therapy session as well. They served as great trial and error runs but no cure yet. Thank you so much.
Dr. Chris
Posted at 00:04h, 16 AprilHi Alexander, almost all “glute pain” is referred pain coming from a disc in the low back. Check out this image (https://www.google.com/search?q=low+back+sclerotogenous+referral&source=lnms&tbm=isch&sa=X&ved=0ahUKEwic6aXzp9PhAhWyzlkKHasyBWIQ_AUIDygC&biw=1641&bih=817#imgrc=mJg2kR6gwv9zVM:).
Assumning this diagnosis is right, you’d have to get adhesion release on the low back. The primary adhesion release treatments for the low back would be the supraspinous ligament (https://www.youtube.com/watch?v=tOgzhYbVpc0). and erectors (https://www.youtube.com/watch?v=4Wc1OrheRdM)
Alexander Zecos
Posted at 07:00h, 18 AprilHello Dr. Chris,
Thank you so much for your response. I saw a chiropractor today at LiveSmart Chiropractic and Rehabilitation and unlike my primary care doctor, plus a certified nurse practitioner, plus my physical therapist, my chiropractor said he believes I actually recently fractured my hip. My chiropractor said he believes because an isometric exercise caused this injury it’s an avulsion fracture. I will be getting X -rays soon. I will get on crutche(s) tomorrow so I don’t cause unnecessary damage to myself. I’ve been toughing it out and things have been very very slowly kinds improving but kinda getting worse at the same time so this diagnosis I got today may have saved me from healing improperly. It’s already been 4 months and I’ve just been limping and walking around with a messed up gait like no biggie. D’oh!
-Alex
Dr. Chris
Posted at 10:33h, 18 AprilHuge Alex. Good – I like a theory with plan of action. Let me know what happens. here for you. <3
Christina T
Posted at 21:26h, 19 JanuaryVery informative article! Would this cause issues with si joint pain? I am constantly having issues when weight lifting with my si joints. Constantly hurting and repeated visits to the chiropractor. Seems to be when I do squats, deadlifts. I know I have some mobility issues as I cannot pull my knees to my chest as well as other limitations. Thank you
Dr. Chris
Posted at 00:44h, 28 JanuaryIn 10 years of practice, I’ve never seen SI joint pain. It’s almost always a disc referring to SI joint and people will finally believe me when they have PERMANENT relief in 3-5 treatments. Stop getting adjusted. Is it giving you permanent relief? (I know the answer). Adhesion release will restore hip flexion as long as your hips aren’t severely degenerated.
skip miller
Posted at 21:00h, 14 FebruaryHi I have been surfing for 40 years..when I stand up I get a sharp pain in my left groin…I have a buldging l4 l5 disc and spinal stinosis..the mri determined I do not need surgery..I had my hips xrayed and there is not arthritis…when I sit or drive for a while and get out my back is stiff..after I walk it loosens up…I did the knee to chest and my good leg goes all the way to my chest and my bad (left) is about 4 fingers off my chest..I feel a pinching pain in my groin when I go further…this has been going on for almost 1 year and I have stopped surfing to see if it heals..what can I do???
Dr. Chris
Posted at 13:13h, 19 FebruaryHi Skip, this could either be a labrum issue (warranting an arthogram of hip) or the L4-L5 disc. The best thing you can do now is take stress off low back over a few weeks to months and see if it gets better. Make sure you’re sitting according to Sit-Slide-Lean rule. See if it recovers. You can also get imaging. This stuff is hard to fix without getting someone to remove adhesion. That’s why people travel from across the country to see us.
Kim Cusick
Posted at 03:06h, 24 AprilMy 11 year old son was diagnosed with spondylolysis in January. After the pain subsided he began physical therapy to learn how to strengthen his muscles. During therapy he was not able to bring his knee to his chest in both legs. He was told to practice that movement at home. It is difficult for him even after weeks of practice. It doesnt hurt. But he just cant do it without help. Is this a side effect of spondylolysis or something more I should look into?
Dr. Chris
Posted at 21:53h, 01 AugustBringing his knee to his chest is putting stress on the spondy.
It’s not a side effect per se, but it makes sense.
I would have him do it more as a test than as practice. It’s more to assess how much stress the spondy is able to take.
If it doesn’t get better in a few weeks to months, I’d seek out more help to figure out why the spondy is so sensitive. He’s too young to be dealing with that.
Kev K
Posted at 20:48h, 31 JulyHi, When I lift my right leg up to my chest, I hear a “clunk” sound come from around my hip area as opposed to a snap/pop sound. If I move my leg outwards and lift the leg again, I don’t hear the sound. There is no pain, but do you know what this might be? I also have patellar maltracking which is not resolving itself by strengthening the VMO and glutes and I think this may be linked. I also sit during the day more than most people. Thanks!
Dr. Chris
Posted at 21:55h, 01 AugustIt’s likely a labrum tear. If you want to know for sure, you’d get an arthrogram.
Patellar maltracking is secondary to hamstring compromise. The next question is why that? Could have multiple causes. I have a blog explaining how to figure out why hamstring compromise is happening, but I can’t find it LOL. I’ll keep looking.
Richard Saunders
Posted at 14:38h, 09 JulyCheers Doc
I am a retired Paramedic who spent most of my 32 year carer using manual stretchers. I have also played hockey since I was 5, still playing and refereeing at age 60. Since Covid I have gone from being on the ice 15-25 times a week to zero. Since I started golfing I have been experiencing 8/10 pain in my left hip going down my leg & into my groin. When I lift my leg and rotate it out it grinds. I fail your thigh to chest test miserably. I do dee an Osteopath on occasion but need to start the 4 week stretching to see if I can improve. I would appreciate your input!
Dr. Chris
Posted at 13:21h, 05 AugustHello my friend, sorry to hear this. Probable hip joint degeneration. The low back could also be involved. It’s really as simple as finding an adhesion release doctor, although there aren’t many of us. Go to integrativediagnosis.com and click find a provider.
Karly Craven
Posted at 12:14h, 28 SeptemberSo I have failed this test miserably. Im a fit and healthy 36 year old woman and it’s getting me down. My hip feels like it gets stuck at the front when I do anything that requires me to bring my thigh to my chest. I’ve had an Ultrasound which showed nothing much but I do have a snapping hip but that’s in an different spot to the front of the hip. possible labral tear so recommended MRI. I had the MRI and no labral tear present, everything about my hip looked normal on the MRI.
I should add I have never had good flexibility in the hamstrings. I’m one of these people who can’t do the splits no matter how much I try. I’m in Brisbane Australia and don’t think we have adhesion release specialists here, maybe they are called something else? I want to get this sorted once and for all.
Dr. Chris
Posted at 18:18h, 28 SeptemberHi karly, sorry to hear. An MRI is 70% sensitive for a labrum tear. An arthrogram is 90% sensitive. So there’s a 3/10 chance the labrum tear was missed. If you’re really suspecting labrum tear, get an arthogram.
There ARE some providers in Australia. Go here.
https://integrativediagnosis.com/find-an-id-provider/
Bota Monkenova
Posted at 11:04h, 24 FebruaryDo I understand correctly that if bringing the knee to the chest is not possible, one should stretch the posterior pelvic capsule and the adductors?
Dr. Chris
Posted at 13:26h, 05 MarchYes, you should “try stretching”. Although if there’s adhesion, it likely won’t work.