

15 Jan Know Your Numbers: Ankle Pain, Foot Pain, and Ankle Dorsiflexion
Without an ankle dorsiflexion (knee to wall test) measurement, don’t bother trying to get your ankle pain or foot pain fixed. ~Barefoot Rehab
So … you have a calf, ankle, or foot problem.
Hopefully, it hasn’t gotten so bad that you have plantar fasciosis or achilles tendinosis.
Do you know how many inches of ankle dorsiflexion you have?
If you don’t, you need to.
The most important test when it comes to measuring the integrity of the leg and foot is ankle dorsiflexion or the Knee to Wall Test.
It is the most functional range of motion for the ankle because as human beings, we walk arguably more than any other activity we do (excluding sitting and sleeping).
Before you push off to swing your foot through when you walk, your ankle approaches your end range of dorsiflexion. Without sufficient range of motion, your body compensates. One compensation is when your hip flexes early to avoid touching the end range of dorsiflexion (contributing towards hip flexor overuse and adhesion). Another compensation occurs when your foot externally rotates (contributing to first metatarsal overuse, adhesion, and risk of bunion) and you walk like a duck.
Quack, quack.
We also need access to ankle dorsiflexion range of motion to squat to maximum depth with an upright chest. Restricted dorsiflexion results in an immature squat (with your chest way over your knees to counterbalance your butt, which is too far back) or the feeling that you are falling backwards.
Three Key Tips to Tip The Scales of Success
Your ankles are on your feet and carry your body around for most of the day when you walk and stand (obviously, not when you sit). Your ankles are load-bearing and work the majority of the day, even when you’re not exercising, running, jumping, or lifting. The load faucet, due to the nature of ankles, drips into your capacity bucket all day long when you’re on your feet.
By comparison, your shoulders, which are hanging freely from your clavicles, are not load-bearing and therefore, recover more quickly than ankles. With shoulder injuries, you can turn the metaphorical faucet off by not using shoulders. You don’t use (load) your shoulders when you sit, walk, or stand.
- Ankles = Load – bearing = work harder throughout the day = difficult to give time to repair.
- Shoulders = Not Load – bearing = work less throughout the day = easier to give time to repair.
As we discussed in Why You’re In Pain, when Load exceeds Capacity, you get pain. When you’re in pain and Load continues to exceed Capacity, you don’t heal.
Key Tip #1: If you’re serious about restoring ankle dorsflexion range of motion or recovering from your calf, ankle, or foot injury, then you need to deload. In this case, that means minimizing walking and especially, prolonged standing.
Key Tip #2: Orthotics are a must when it come to load management. In some cases, an over-the-counter insert can decrease load and reduce symptoms. In our office, we use the best orthotics out there, Sole Supports (FYI – We get nothing for telling you how amazing these supports are). They’re wonderful orthotics casted seated in a maximally supinated position, thus cushioning the arch with each step you take. A non-maximally supinated orthotic does not cushion the arch like this. The orthotics take into account your body weight and foot flexibility as well, which makes them quite individualized.
Key Tip #3: Stretch the right tissue. Too many people waste their time stretching the calf with their knees straight. The gastrocnemius rarely ever has adhesion and does NOT stop the knee to wall test. It’s best to stretch the ankle with the bent. See the “Specific Dysfunction” part below about which tissues are relevant.
Ignoring these key tips could mean that you’re doing all of the right stretches and getting all of the right treatment and if your range of motion isn’t increasing, you are simply not giving your tissue a chance to recover and loosen up.
Mobility: Knee to Wall Test | Ankle Dorsiflexion (AD)
Don’t judge my orange SkyZone socks. First, that place is like heaven for adults who want to peg kids in the head with dodgeballs, as I did and wrote about in The Good Body Project. Second, the socks come with grips on the soles of the feet that give you extra traction when you’re trying not to slide across wooden floors. Super comfy!
The ability to touch a wall with your toes 5″ away from a wall and your heel down is something that anyone should be able to do, when healthy. The “Knee to Wall Test”, or in mechanical terms, ankle dorsiflexion, will let us know if you have that ability.
What do I need to Measure this Test? In our office we use white blocks in 3″, 2″, 1″, and 1/2″ increments. It’s easier for patients to visualize their range of motion with a 3-D block. You can just as easily use a ruler on the ground.

What is the Knee to Wall Test assessing? The mobility of your calf, ankle, and foot integrity. These structures include bone, ligaments, tendons, cartilage, and muscles.
What Specific Dysfunctions are relevant here? Unlike the lumbar spine that tends to accumulate many structural dysfunctions, the ankle tends to be structurally healthy. That’s good news for us! This means that the majority of individuals with restricted ankles should be able to increase range of motion except when trauma has caused permanent damage. When dysfunctions are present, pathologies around the mortise joint are the most common and what would limit this range.
Relevant muscles include:
- tibialis posterior – the stretch is in the middle of the calf, deep.
- flexor digitorum longus – the stretch is in the medial portion of the calf, deep.
- flexor hallucis longus – the stretch is in the lateral calf, deep.
- posterior tibiotalar ligament – If this is problematic, you’ll feel a pinch on the front of the ankle. This ligament cannot be stretched or mobilized. The only way to affect this tissue is with a manual therapist who would take the small edge of a finger and put it under the malleolus to treat it.
- posterior talofibular ligament – see “posterior tibiotalar ligament” above.
- soleus – This muscle, while relevant on occasion, is not as significant as the 1st 5 structures above. What this means for you if you’re mobilizing, go as deep as possible. The structures above are deep to the soleus. Use an object with a smaller surface area – lax ball, or even a golf ball – than an object with a larger surface area – foam roller.
Completely irrelevant muscles include:
- gastrocnemius (This muscle is stretched with the knee straight. Don’t bother stretching this muscle as it almost never has adhesion.)
What You Need to Know: A calf stretch during the SLPF Test has a completely different physiologic cause than this test. It’s nerve in the former, muscle in the latter.
How to Test: Take your shoes off. Put a ruler against the wall. Start with your toes against the wall, standing on top of the ruler. Heel down. Keeping your heel down, move your knee straight forward toward the wall without letting your knee cave in towards your first toe. If you knee touches the wall with your heel down, you have that range of motion. Move your toes 1″ away from the wall at a time, continuing to be sure that your heel is down and your knee doesn’t cave in. The last range of motion before your heel is about to lift or when your knee just barely touches the wall is your Ankle Dorsiflexion Range of Motion.
Watch the three minute video below if you’re of a visual person.


Write this number down. Any mobilization, stretching, or treatment interventions are attempts to increase this number. If the number isn’t increased after a month, you’re wasting your time.
PASS:
A pass for this test is the ability to touch a wall with your toes 5″ away from a wall and your heel down (best visualized from the side). When observed from the back, the knee should be over the 2nd toe. Notice, for integrity’s sake, I only have 4.5″ of range of motion in the picture below titled “Passing End Range of Motion”. I want to show you what a full range of motion looks like. For the passing test’s sake, imagine another 1/2″ block thrown in there.


- Range: 5 inches (don’t be confused by my 4.5 inches of maximum range – I fail this test).
- Effort: Fast and easy.
- Symptoms: No symptoms, including stretching.
FAIL – LOW RISK:
A fail is any range of motion between 3″ – 5″ with the heel down, the knee touching the wall and the knee over the 2nd toe. For the athletes out there, the lower end of the spectrum here is the minimum amount of dorsiflexion needed to perform a hip width, toes slightly out, Olympic-style squat. In this case, 3″ was my personal measurement, given the length of my femur (thigh bone), tibia (weight-bearing leg bone), and foot. Your body is different than mine, so your number will likely be different as well.
- Range: 3 inches – 5 inches.
- Effort: Fast and easy.
- Symptoms: Because your range of motion is limited, some tissue will be stopping your range of motion, which means that you will likely feel a “stretch” sensation somewhere in the calf, posterior ankle, or foot. You could also have an impingement (“pinching sensation”) in the front the ankle, which would indicate that the posterior tibiotalar ligament or posterior talofibular ligaments are adhesed. Don’t even bother rolling out if this is the case. See a manual therapist to remove the adhesion in those ligaments. If you have pain, you have a problem and you should either rest before you test again or see a qualified therapist.
FAIL – HIGH RISK:
A fail, with an individual having no business doing any non-essential walking or exercise, is anything less than 3″ with the heel down, the knee touching the wall and the knee over the 2nd toe.
- Range: Less than 3 inches.
- Effort: Slow and cautious, indicative of “protective tension” and “red-lighting” from the central nervous system. This protective mechanism occurs when tissue is damaged and the body is subconsciously protecting further load from occurring to the damaged tissue. If you feel a “stretch” when combined with this slowness, the cause of the “stretch” is actual muscle contraction or “protective tension”, not the lengthening normally thought of as a “stretch”. This means that if we cut look at the tissue on a microscope, we would see the muscle’s active units, the sarcomere, sliding past each other (indicating contraction), not moving further away from each other (as seen in a stretch).
- Symptoms: See above in the “Low Risk” section. If the range is this bad, it’s possible that this range of motion has been restricted for a long duration of time, which means that you’ve been compensation for a long time as well. Knee and hip symptoms during this test indicate that you should really consider getting help.
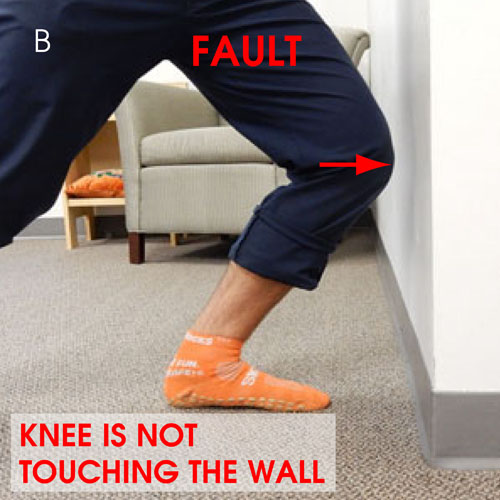
Movement Faults:
If your heel lifts (see A), if your knee can’t touch the wall (B), or if your knee caves in (out of alignment with the 2nd toe), you’re toes are too far from the wall and you need to move closer.



I Know My Numbers – What do I do now?
Insanity: doing the same thing over and over again and expecting different results. ~Albert Einstein
There are a plethora of mobility and stretching resources out in the interweb for you to experiment with to improve your ankle dorsiflexion. I like this post with 7 advanced mobility exercises. It is not our intention to give prescriptive answers, simply to bring awareness to where your body currently is in time. One meta-analysis done in 2006 supports the notion that static stretching from 5-30 minutes can create small improvements in ankle dorsiflexion.
Use whatever tools you’d like to use for a month, stretching about from 5-30 minutes a day, for 3 days a week, for a month.
After a month, re-test.
If you’ve gained range of motion, wonderful! Wash, rinse, repeat, and continue stretching.
If you’re no more flexible or mobile than you were before, STOP THE INSANITY AND THE STRETCHING! 
It’s now time to see a Manual Adhesion Provider or Active Release Technique Provider to diagnose your condition and potentially remove the adhesion in relevant tissue to restore your mobility before you go on layering strength on top of unhealthy tissue.
Below, our clinical assistant Sharon and I treat a patient with chronic ankle pain’s flexor hallucis longus. This muscle is one of the primary tissues responsible for restricting ankle dorsiflexion.
Once you’ve gotten your Ankle Dorsiflexion range of motion to as close to 6″ as possible it’s time to strengthen. I really like this comprehensive guide for strengthening the calves and shins to increase your capacity so this restriction in joint range doesn’t happen again.
Want to test the rest of your muscles and joints? It’ll only take 2 minutes per test, but you need a friend to help.
- A Screen for the Low Back, Hamstring, and Sciatic Nerve – Touch Your Toes Test
- Low Back Pain – The Super Simple Pencil Test
- Sciatica or Hamstring Tightness/Pain – The Hamstring Stretch Test
- Wrist and Elbow Pain – The Wrist and Finger Extension Test
- Knee, Cartilage, or Meniscus Pain – Face-Up Heel to Butt Test
- Quad Tightness/Pain – Face-Down Heel to Butt Test
- Hip Flexor Tightness/Pain – Lunge Stretch Test
- Hip Pinching or Groin Tightness/Pain – Thigh to Chest Test
 What are you ankle dorsiflexion numbers? Please share range, effort, and symptoms below and we can discuss what you should be doing to restore musculoskeletal integrity.
What are you ankle dorsiflexion numbers? Please share range, effort, and symptoms below and we can discuss what you should be doing to restore musculoskeletal integrity.

Know Your Numbers: Ankle Pain, Foot Pain, and Ankle Dorsiflexion Test | Primal Docs
Posted at 20:51h, 15 January[…] Know Your Numbers: Ankle Pain, Foot Pain, and Ankle Dorsiflexion Test […]
Maria Sexton
Posted at 18:17h, 19 NovemberI was told I suffered a grade 3 ankle sprain almost 6 weeks ago. I stumbled across this site and out of curiosity tried the knee to wall test. My range was less than an inch and at 1 inch there was pain. My orthopedic doctor has yet to even lay hands on my ankle. I am to begin physical therapy in 2 days and I am afraid of pain or accidental injury from improper diagnosis. My ankle, when I stand and put weight on it slides in and down making my foot look like it is flattening out. This is also very painful. The pain is on the outside, Inside and in front but above my ankle as well as below my knee on the outside of my calf.
Dr. Chris
Posted at 11:12h, 20 NovemberHi Maria, the good thing about injuries like yours is that the diagnosis is usually correct. Based on what you mention about your symptoms and how the ankle moves, it sounds correct. You should keep doing this test to assess how you are progressing. The goal is 6″ of range of motion. If PT doesn’t help you get there, you may need a manual therapy specialist. Let me know how I can support you.
Maria H Sexton
Posted at 21:00h, 10 FebruaryHi Dr. Chris. I wanted to update you since my last post. After 9 weeks of no pain/stability improvement I had an MRI of my right ankle done. Turns out I sustained grade 2 sprains of atfl, anterior and posterior tibiotalar components of the deep deltoid ligament. Grade 2 sprain of the syndesmotic ligaments as well, but here is the kicker: mildly displaced vertical fracture of posterior malleolous w/ persistent (don’t know what this means) hypointense fracture line extending to articular surface and significant associated marrow edema. Marrow edema extends to the syndesmosis. Again, this is 9 weeks AFTER the initial injury and the MRI report stated the fracture was in the earliest stage of healing. I’m assuming this is because of walking on it , well limping on it. As of yesterday I was allowed to put away my crutches and focus on proprio-something, learning to keep the ankle stable right? The pain has decreased significantly but my tibia still hurts/ aches and the ligaments still sting a bit.
Dr. Chris
Posted at 13:55h, 12 FebruaryThis is awesome Maria. We have more data that now makes your pain, stability, and functional ROMs make sense. Yes, the walking is likely the reason why you weren’t healing (your body can’t heal and take more stress at the same time). Now, the plan is to use your crutches and let it heal as much as possible. I would do some really gentle “loading” (or putting stress on it) by putting your foot on the ground and gentle re-creating the knee-to-wall test to encourage blood flow into all of the ligaments. Less is more here. It’s not a workout. I’d literally start doing this maybe twice a day for 20 seconds, performing 2 or 3 reps. Let ease be your guide. If it’s painful or feels off, stop. If it starts feeling better after a week, do more. If you’re overweight or have any metabolic conditions, know that those factors are also inhibiting your progress. You should make sure you’re getting as much nutrition in your body as possible (grass-fed meats, wild-caught fish, colorful vegetables, bone broth, etc). Hope this is helpful?
Katie
Posted at 20:59h, 14 SeptemberWhat should I do? On my left leg I just got 1cm (never broken before) on the right with several metal implantats I am not able to touch the wall with my knee even if touch the wall with my toes without Lifting heels. Is this even managable?
Dr. Chris
Posted at 18:03h, 15 SeptemberHi Katie, yeah, that’s very bad. It’s hard to say what’s restricting you. You’d need to have an in person exam with an adhesion specialist to figure it out to set your ankle up for long term health.. You can find one at integrativediagnosis.com.
Kim Ray
Posted at 20:15h, 17 MarchI had Lapiplasty Bunionectomy on my right foot Dec 17, 2019. Recovery progress seemed good until I realized I couldn’t dorsiflex my foot while my leg was straight, weight bearing or not. I’ve been trying to mobilize the ankle and stretch the calf and have gained a little bit of dorsiflexion but now the front of my ankle has pain almost all the time. I did the test and got exactly 3” slow and cautious. Any suggestions would be appreciated.
Dr. Chris
Posted at 23:14h, 17 MarchHi Kim, it’s hard to say. But you can dorsiflex your foot when your knee is bent? If yes, would likely be a gastroc issue, potentially adhesion. If no, then it sounds like there’s an impingement in the mortise joint. Could be a bony joint issue, or more likely, there’s adhesion in flexor hallucis longus, followed by tibialis posterior, flexor digitorum longus, and posterior tibiotalar ligament. You can try sitting with your calf on a golf ball or lax ball and finding sore spots. I wouldn’t stretch it as you could make it worse. Best option is to find an Integrative Diagnosis doctor to remove adhesion. Hope that helps.
Kim Ray
Posted at 20:19h, 18 MarchDr Chris,
Thank you for answering my question, however I need to know what I can do for myself at home right now as I won’t go to a Drs office right now during the Pandemic unless it’s critical. I believe I am able to dorsiflex with my knee bent but I don’t know how to measure it to be sure.
Dr. Chris
Posted at 21:16h, 18 MarchIf you did this test the way we describe it, then the knee would have to be bent. Try the lax ball trick. Let me see if I can film a video and I’ll upload it.
Kim Ray
Posted at 15:00h, 19 MarchDr Chris,
Thanks, I will try that.
Is there a functional difference between being able to dorsiflex against the floor like while doing the test and dorsiflexing under my own power without assistance? I can force my foot into more dorsiflexion both straight legged and knee bent than I can achieve in the air without assistance.
Dr. Chris
Posted at 01:56h, 20 MarchIt’s better (healthier) that you can do it with foot on floor. It’s more practical. Ideally, you’d be able to do it in air without assistance. Obviously, suggests something isn’t right.
Richard
Posted at 22:43h, 13 AprilHi Dr Chris. Thanks for the dorsi flexion guide.
It’s 8 weeks since I sustained a suspected grade 2-3 ankle sprain with an avulsion.
I can walk fine without a limp.
My measurement doing this exercise is 2 inches. I only measured it today but I’ve been doing this exercise for about 4 weeks. I think I have probably progressed about an inch and a half since then.
Any advice on how I could progress with this would be appreciated.
Kim Lewis
Posted at 01:55h, 06 AugustHi ! I broke my tibia in several places as well as my fibula skiing almost 8 months ago abroad. The tibia was repaired with a nail. The fibula was not touched. I have partial union of the breaks in the tibia and non-union in the fibula (which is hugely painful). My local ortho said repairing the fibula isn’t worth it (?) and I’m now doing my best to get back to my normal (very active) life while trying to manage the pain. I can somewhat successfully work out (all low impact – I cycle on my peloton!) – no jumping, running, skipping, lateral movement – which is torture for me as a basketball player!!! Who knows if skiing is in my future! just came across your material – very helpful! My dorsiflexion has been terrible – less than 2” for a long time – no improvement in well over 4 months. Pain deep in my ankle, front of ankle and all up the outside of my leg. I know part of this is where the unhealed break is… I also notice that my calf doesn’t seem to engage at all (maybe minimally). You’ve probably seen this before…and was hoping for some advice. I do think that unlocking my ankle will help (at least mentally!). Thanks!
Kim Lewis
Posted at 02:08h, 06 AugustHi ! I broke my tibia in several places as well as my fibula skiing almost 8 months ago abroad. The tibia was repaired with a nail. The fibula was not touched. I have partial union of the breaks in the tibia and non-union in the fibula (which is hugely painful). My local ortho surgeon said repairing the fibula isn’t worth it (?) and I’m now doing my best to get back to my normal (very active) life while trying to manage the pain. I can somewhat successfully work out (all low impact – I cycle on my peloton!) – no jumping, running, skipping, lateral movement – which is torture for me as a basketball player!!! Who knows if skiing is in my future! just came across your material – very helpful! My dorsiflexion has been terrible – less than 2” for a long time – no improvement in well over 4 months. Pain deep in my ankle, front of ankle and all up the outside of my leg. I know part of this is where the unhealed break is… I also notice that my calf doesn’t seem to engage at all (maybe minimally). You’ve probably seen this before…and was hoping for some advice. I do think that unlocking my ankle will help (at least mentally!). Thanks!
Dr. Chris
Posted at 12:00h, 06 AugustTough Kim. You may have adhesion which would help getting it removed. But it’s likely the break may prevent the range from ever coming back. It’s difficult to say more without seeing you in the office. You’ll have to use your discretion with what surgeon and manual therapists tell you.
The Truth About Plantar Fasciitis (and Arch Pain)
Posted at 12:56h, 19 January[…] which is often very true with restricted ankle dorsiflexion and plantar flexion (see below – Measure your ankle dorsiflexion through the directions here). Tissues can be tight for various reasons that warrant further detail to resolve (ie. muscle […]
Do You Trust Your Doctor & Advanced Pain Management: The Research on Expert Intuition
Posted at 15:39h, 08 February[…] sustainable improvement in her functional range of motion (her restricted and relevant test is ankle dorsiflexion, showing 2.5″ on both sides) and no improvement in her capacity upon walking barefoot. […]
Foot Positioning in the Squat and Ankle Dorsiflexion Range of Motion
Posted at 23:38h, 20 April[…] I already showed you how to measure your ankle dorsiflexion here. […]
Know Your Numbers: The Thigh to Chest Test
Posted at 20:58h, 01 June[…] awaiting 30 days from now to reassess, you might as well get baseline measurements for your ankles and your low […]
Know Your Numbers: The Lunge Stretch Test
Posted at 14:28h, 15 June[…] 30 days from now to reassess, you might as well get baseline measurements for your hip flexion, ankles and your low […]
Sally M
Posted at 21:34h, 12 JulyI have roughly minus one inch of dorsiflexion on my right foot (knee roughly one inch from wall when toes touch wall). I run about 30 miles a week and feel fine except when running uphill, in which case the arch of the right foot feels strongly overstretched to the point of pain. The left foot has positive dorsiflexion of about one inch and feels fine when running. I tried daily calf stretching (both with straight knee and bent) for a few months but dorsiflexion didn’t improve. I felt no stretch in my ankle, just compression at the front of the foot. Is there any way to compensate for lack of dorsiflexion when running, since it doesn’t seem to be improving.
Dr. Chris
Posted at 21:57h, 12 JulyHi Sally, Unfortunately, there is not a way to compensation for a lack of dorsiflexion. When you run, you need more dorsiflexion than 1″. My recommendation is that you stop running, or at least, stop running so much. Because you don’t have 100% capacity in your ankles, your mileage combined with your greatly diminished capacity will only worsen the ankles quickly and surely, other joints upstream (knees, hips, low back). Only time will tell. Riding a bike would take the ankles out of the equation. Is this something you would consider?
Of course, the other option is to find a myofascial worker who can help you regain that range of motion. If you feel compression in the front of the joint, the posterior ankle ligaments are likely involved. There is NO way for anyone to stretch or mobilize these tissues without a skilled provider.
I hate to be the one to give this recommendation. Know that my perspective comes from wanting to see you able to walk ( and run if you have to) decades down the road. That’s why I make this recommendation. Let me know your thoughts.
Sally
Posted at 06:48h, 02 JuneI’ve switched to barefoot running (in fact I’m barefoot or in Xero sandals 100% of the time) and feel great! Still get a negative result on the wall dorsiflexion test on my right foot, but not having foot pain any more.
Dr. Chris
Posted at 11:33h, 02 JuneWonderful Sally.
With 1″ of dorsiflexion, you should continue to be mindful over the months to years how your feet and calves feel. Barefoot running puts MORE load on these structures (generally), not less. But if you’re having more relief, whatever tissue was causing your pain is being loaded less, at least in the short term.
If you’re really mindful and you do get a little symptom here or there, respecting those symptoms will help you to do the right thing by whatever is damaged.
Sally
Posted at 12:55h, 02 JuneI have MINUS one inch actually on my less flexible side…
Dr. Chris
Posted at 15:59h, 02 JuneYeah. You have a giant mass of an iceberg brewing underneath the surface, you just can’t see it yet. Please keep your running down to low volume and introduce intervals if you’re going to run at all. I’d be really surprised if 6 months from now, you’re still running barefoot like this.
Forgive me for being the bearer of bad news, but I’d rather you get reality than false statements.
Sally
Posted at 08:41h, 16 JuneThat’s exactly what you said last year. I’ve increased mileage with no pain. I get that you’re trying to make money here, but why lie?
Dr. Chris
Posted at 11:28h, 19 JuneHi Sally, I’m glad you’ve been able to increase your mileage with no pain. It’s very common that over months to a few years, people can increase the amount of activity they have, even with severely restricted joints. So I’m not surprised you have no pain. My previous messages are warning signs that you will have growing pains over the next few years due to the 1″ of ROM. The more you monitor your activity, take care of your soft tissue, and understand “what’s going on underneath the car’s hood,” the more you’ll be able to prevent this. My intention in replying again is bringing this mindfulness to your running, not to upset you in any way. I apologize if I’ve done so.
As far as trying to make money, I’m not quite sure what you’re talking about. Do you think I”m trying to get you to NJ as a patient? I don’t know where you live in the world but that’s usually not possible for people.
Know Your Numbers: The Face-Up Heel to Butt Test
Posted at 17:49h, 16 July[…] now to reassess, you might as well get baseline measurements for your hip flexion, hip extension, ankles and your low […]
Seth Hamilton
Posted at 19:01h, 22 DecemberI have a dorsiflexion of 1 1/8th inch. I “fractured” my talus in Feb 2015, and it doesn’t seem to be getting any better. Any suggestions to restore my range of motion if the exercising doesn’t work?
Dr. Chris
Posted at 14:34h, 27 DecemberHi Seth, I’m sorry about the fracture. Before asking your question, the real question is, “What is stopping your dorsiflexion at 1 1/8th inch?” If it’s soft tissue, you can gain that ROM back. If it’s due to the fracture, the talus, and a bony stop (imagine a wallet in a door hinge), then you cannot get it back.
Let me ask you a few questions.
– Did you need surgery?
– Do you have the images of the fracture?
– Did your doctors tell you if they thought you would get that ROM back?
– Have you had a skilled manual therapist feel your deep calf tissue (or posterior ankle ligaments) to determine if they’re pulling tight and stopping that ROM?
Answer those questions, feel free to send me any imaging or reports you have (delight [at] barefootrehab [dot] com), and I’ll take a look for you.
Dean Webber
Posted at 14:20h, 30 AprilReally glad I found this site! I have roughly 2″ dorsiflexion on both ankles, and have tried visiting numerous chiropractors and physios with no improvements (over a year!). It’s really hard trying to find a decent practitioner! Besides coming to your clinic (wish I could but I live in Japan!) could you give me some tips on how to tell a good practitioner from a lazy one. Thanks
Dr. Chris
Posted at 22:17h, 30 AprilHi Dean! Glad you enjoyed the post. Sure, here are a few tips:
1. Does the doctor have testimonials and case study proof of range of motion gains?
2. Does the doctor claim to fix everyone (100% of the time) or are they realistic about the gains that can be made (expressing humility and realism – some people won’t have increases in ROM based on structural damage or overuse).
3. If you do see a doctor and you don’t notice any range of motion changes in 5 visits, find another doctor.
Hope this is helpful.
Mary Ann Johnson
Posted at 16:49h, 03 MayI have bilateal foot drop. I had back surgery of decommpression and fushion of L4 L5 and,S1 with hopes of it helping but no improvement. My legs, hips and everythung below waist are weak. I’m doing physical theraphy with no improvement. I had an emg and dr said findings could be consistent with cidp. What kind of dr do I need to go to. I have been in wheelchair since Christmas of 2016.
Dr. Chris
Posted at 17:09h, 03 MayHi Mary Ann, I’m so sorry for your struggles. What happened around Christmas 2016? Was there any trauma? Were you really stressed out? Were you doing anything with your body prior to that time? Maybe a new workout or work activity?
If your doctor is right, CIDP is a neurological condition. You should see a neurological specialist.
Physical therapy wouldn’t work because while you’re “weak”, it’s not a “muscle weakness” issue but a “nerve isn’t activating muscle” issue. So that makes complete sense.
Someone like me wouldn’t be able to help you UNLESS the nerve part was managed.
Hope this is helpful. If I can do anything else, please let me know.
BarefootRunner
Posted at 17:27h, 29 November“The ability to touch a wall with your toes 5″ away from a wall and your heel down is something that anyone should be able to do, when healthy.”
These numbers simply don’t work for shorter people. My foot length is 24cm. Heel-to-knee length is 44cm. To get my knee to touch a wall with my toes 5″ (13cm) away would require an angle of arccos((24+13)/44) = 33 degrees between foot and shin, or the ability to flex the foot 57 degrees upward from perpendicular to the shin. That seems like a rather extreme amount of flexion.
“A fail, with an individual having no business doing any non-essential walking or exercise, is anything less than 3″ with the heel down, the knee touching the wall and the knee over the 2nd toe.”
I measure zero on the wall test when fully warmed up. I’ve spent my life walking, hiking, and dancing and I’ve been running for several years. During 2017 I transitioned to barefoot running and am currently at 40km a week with no issues.
Dr. Chris
Posted at 17:57h, 29 NovemberHey there,
I agree that the numbers don’t work for much shorter or taller people. But it works for most people.
I don’t know how old you are. But with 0″ of dorsiflexion in this test, I will make 3 assumptions that may not be true:
1. You’re genetically gifted when it comes to having strong connective tissue.
2. You’re probably healthy in your other joints.
3. It’s likely only a matter of time before something breaks down in your ankle or foot.
But yes, I agree that 5″ isn’t passing for every individual.
John K
Posted at 19:46h, 30 JanuaryHello,
I have rupture my Achilles tendon in Mar 2017 and had surgery in Apr 2017. My surgery was the PARS with the Speedbridge Midsubstance anchors to the heel. My doctor said that this surgery involves fiber wires anchored to the heel therefore my dorsiflexion is harder to regain. I’m 10 months post surgery and my dorsiflexion is only 2″ from the wall. Can you recommend exercises that can help stretch my achilles to regain my dorsiflexion ?
Thank you so much.
Dr. Chris
Posted at 22:13h, 01 FebruaryHi John, I’m sorry about the injury. I don’t know if “fiber wires” are elastic or not. When the surgeon said dorsiflexion would be “hard to regain”, is it even possible to regain? Before you do anything, I would ask him if this is possible and potentially ask if he has any patients who have had the same surgery who did regain this range. Ask if you can speak to him/her. My humble opinion, now, is that it is not regainable. Let me know what he says?
John K
Posted at 19:09h, 06 FebruaryHi Dr Chris, Thank you for your reply. These fiber wires are not elastic, here’s a link to the exact surgery that I had https://www.arthrex.com/resources/video/aIzAyy_bb0CgmwFBFC30hw/achilles-midsubstance-speedbridge-knotless-achilles-repair. Yes, my surgeon said it was possible with stretching and exercises. I’m now 10 post surgery and I need some more ideas of exercises at home or local gym. My PT session have ran out therefore I’ll have to do these on my own. Thank you.
Dr. Chris
Posted at 19:19h, 06 FebruaryGot it John. I suggest trying this: https://performancecarerx.com/corrective-action-ankle-dorsiflexion/
Report back in with me if you do it?
Sophie Cowper
Posted at 09:57h, 12 AprilHi, I have a negative figure on left foot which has a bone spur on the heel which I feel is restricting me. Is there any way I can increase dorsiflexion, as surgery is a last resort. Thanks.
Dr. Chris
Posted at 13:36h, 12 AprilHi Sophie, what do you mean by a “negative figure”? Where is the bone spur? read exactly what the x-ray or MRI report says. Typically, bone spurs happening at the heel (where plantar fascia inserts) wouldn’t restrict this range of motion. It’s not involved with any of the muscles that could be limiting the range of motion.
So the suspect that is limiting your range is still unknown.
What is your range?
Tammy Romer
Posted at 22:24h, 19 JuneDr. Chris,
Hi! I am 14 weeks post-op plantar fascia release, bone spur removal, and tarsal tunnel release surgery. Since surgery, I have lost dorsiflexion. I do not know what my numbers were before surgery but I know that I did not recognize it as an issue. Since surgery my measurement in PT is 10 degrees. I have been going to PT three days a week for 10 weeks with zero improvement. I attempted your easy measurement trick and with my toes up against the wall I could not get my knee closer than 4 inches to the wall. Since surgery, I developed a DVT and was diagnosed with complex regional pain syndrome. I am told that this CRPS is the cause of my lack of dorsiflexion but not given any other information. Any thought or suggestions you may have would be greatly appreciated. I want to get back to work but between the nerve pain and mobility issues I’m just not sure how that will happen. Thanks in advance!
Dr. Chris
Posted at 10:57h, 20 JuneHi Tammy, I’m sorry for your struggles. 4″ is 64% function. Not horrible, but could be a lot better. 30 Treatments is WAY to many to not have improvement. CRPS is 100% not the cause of your lack of dorsiflexion. It tells us nothing about what tissue is stopping your range of motion. Now, with the surgeries you had, it’s very possible that you won’t be able to recover that range due to structural (joint, cartilage) damage of the joint, kind of like gears in a machine that are tinkered with and can’t be repaired. I’d try to find the most precise myofascial therapist you can find near you. Ideally, they’re an Integrative Diagnosis provider. They’re taught to get range changes in 3 treatments or less and can often diagnose what the cause of your restricted range is. Let me know your thoughts.
kartik wadhawan
Posted at 15:12h, 07 Octoberi am having ankle dorsiflexion problem i am a gymnast from india i am having 4″ movement in my right ankle with little effort and 5.5″ in left easily wall test i cannot take deep landing if feel like sumthing is torn from inside i have pain in front little to right side near the bone and the pain is painfull i have been doing some balancing and streching exercise and move i am doing so strengthening but i cannot see any improvement i can feel the stiffness with i sit in squat position with both legs join please can you help me with somthing
Dr. Chris
Posted at 19:56h, 07 OctoberYou need to find someone to treat you Kartik. You have a problem. Hopefully, it’s adhesion. You could have cartilage damage in the location you describe. There’s nothing you can do besides treatment. I’m sure you’ve tried a lot already!
Mike
Posted at 20:39h, 15 OctoberHello Dr. Chris,
Glad I found this website. 16 months ago I fractured my calcaneous and had 17 screws and a plate put in the heel. A year after the injury I rushed back, and wound up getting posterior tibial tendinitis. After a few weeks of rest, I started to see a PT. We have been doing joint mobilizations to restore my joint mobility/dorsiflexion. There has been a massive improvement and I’m around 4-4.5” once I’m warmed up, but still feel some pinching at times in the Posterior tibial tendon (although no inflammation). It’s been 12 weeks. I also get a pinch in the front of my ankle at times too. I saw you don’t recommend Graston for the post tib tendon…what would you recommend? I feel like I need something other than just joint mobilizations.
Thank you for your time.
Dr. Chris
Posted at 11:13h, 16 OctoberHi Mike,
An instrument can’t reach the tibialis posterior muscle. Although it can reach the tendon on the bottom of the foot by a skilled practitioner. i recommend you get someone who can use an instrument on the bottom of your foot and his/her hands in your calf.
I don’t ever care what someone’s range is after warming up. What matters is what your range is when cold.
Where exactly is the pinching?
Sole supports orthotics will be helpful too. Tibialis posterior is responsible for holding arch up and it’s essentially overloaded if you have a true tendonitis. If your symptoms get BETTER with warming up, you also have tendinosis there.
Bailey Harvey
Posted at 23:14h, 26 OctoberI injured my ankle playing basketball 3 months ago. I landed on someone’s foot after grabbing a rebound and my ankle inversed and dorsiflexed to the extreme. Soon after this incident (a week) I hiked about 30 miles on my bum ankle and I tried to return to sports after a month of my injury. My ankle is no longer swollen, and I am waking normally. I iced and did ankle exercises till now but I am still having problems putting my knee over my toes. I can get my knee to my toes but never further, and I feel pain along the posterior medial portion of my ankle when I try to push my ankle to my toes and past that point. I am a 20 year old who leads a very active lifestyle. What is my injury specifically? And what is your advice for combatting this injury?
Dr. Chris
Posted at 02:10h, 27 OctoberIt’s hard to say Bailey. The posterior medial ankle houses the deep ankle stabilizing muscles (tibialis posterior, flexor digitorum longus, and flexor hallucis longus) as well as the posterior tibio talar ligaments. You also could have damaged the cartilage or mortise joint thehre. Have you seen anyone to check this out? The best way to combat this is to find a specialist who knows what they’re doing. An MRI would provide information. Someone who can feel tissues can tell you how bad they’re adhesed or damaged. I hope this helps.
Bailey
Posted at 14:00h, 27 OctoberI will see a specialist as soon as I can, thank you for your help!
Dr. Chris
Posted at 20:02h, 27 October: ) Let me know how it goes brother.
morteza
Posted at 18:59h, 19 NovemberHello and thanks for your advice
I am a soccer player who suffered ankle sprain and ankle sprain 9 months ago, and I already have ankle limitation after surgery.
I can run but the starter is not like before ……. after running … at home, I get cramps in the ankle area
My ankle bends to the front most likely
Evaluating Ankle Dorsiflexion
To assess if you may have poor ankle dorsiflexion
Dr. Chris
Posted at 11:57h, 20 NovemberHi Morteza, what are you asking exactly? Can you be more clear?
Rae
Posted at 06:08h, 25 NovemberI am at less than 2” in ankle knee to wall test on right side and 3 on my left. Shock therapy, gestard tools, fascia massage, chiro and physio. Need diy stretches seeing as I’m not able to stretch per say
Dr. Chris
Posted at 21:41h, 25 NovemberHi Rae, I recommend you check out Active Life Rx’s Bulletproof Ankle program. This is the best program I’ve found to increase this range by yourself. Let me know how it goes. https://performancecarerx.com/bulletproofrx-ankles/
Emma
Posted at 12:52h, 13 JuneI only could do 2inches!
I felt pain in the front of my foot when I did the test.
I am 25yrs old and have sprained both ankles multiple times over the years. It has been 4years since my last sprain.
I don’t do any regular exercise. I am unable to complete a full squat as I can’t bend my foot, i have attempted multiple times and it won’t allow me to drop down.
On plantar flexion, it almost feels like it hyperextends. My physio has previously said I hyperextend all of my limbs..
Would appreciate some recommendations that I can do while I wait to locate a manual adhesion provider.
Dr. Chris
Posted at 21:19h, 13 JuneHi Emma, if you have 2″ of dorsiflexion, but full plantarflexion, you’re likely experiencing an impingement. The adhesion provider will likely need to treat the posterior tibiotalar ligament and posterior talofibular ligaments primarily, and tibialis posterior, flexor digitorum longus, and flexor hallucis longus secondarily. In the meantime, avoid movements that put you into dorsiflexion as you don’t have access to it. You can try some lax balliing of the calf to see if that improves the range and symptom.
Emma
Posted at 23:34h, 13 JuneHi Dr Chris, thank you for the quick response! I will find an adhesion provider.
Dr. Chris
Posted at 19:58h, 02 July: )
Mike M
Posted at 07:00h, 07 NovemberMy wife runs marathons and suggested I need to start an exercise routine. I tried to work out with her, but she told me to stop because my posture and form were “terrible.” I tried the wall test and cannot touch my knee to the wall without my heel coming up even with my toes against the wall. If I bend my knees at all while standing up, my heels start to rise. I assume this means I have almost no ankle dorsiflexion. My wife and I were hoping I’d be able to start running with her, however, when I run I am basically running on my tippy toes. There are some times I cannot even bring my heel all the way down to the ground.
My wife suggested I find some exercises to improve ankle range of movement. In addition, I am duck footed so it takes effort to get my feet pointed straight. When I point my feet straight (say when I’m in a picture), you can feel a major tightness in the sides of my legs just to hold the feet straight. I cannot turn my feet inwards at all. I am not sure if that affects anything or not.
Dr. Chris
Posted at 00:46h, 28 JanuaryHi Mike, with 0% function in the ankles, if you chose to ran, you’d DEMOLISH your ankles. Please don’t. Try Active Life Rx’s Ankle Mobility program. If that doesn’t work, you’ll have to see an adhesion specialist.
Kylee Underwood
Posted at 21:12h, 12 DecemberI’ve been trying to improve my squats for a long time. I’ve got some lovely hip and SI joint issues…and I think it may have stemmed from having ankle mobility issues. I sprained my ankles multiple times years ago in my rock-climbing years….and now at 32, I’m only getting a score of about 1″ on my left ankle and 3″ in my right ankle! I feel dang defeated (de-feeted perhaps BAHA!) Anywhooooooo…there are no providers near me, so I’m wondering what you’d suggest. I work out 4-6 days a week from yoga, running, and weight-lifting. How can I get over this barrier?!
Dr. Chris
Posted at 00:47h, 28 JanuaryHmmm, I’d avoid end range dorsiflexion. Of course, you can try stretching for a month. But most often, that doesn’t get mobility back if you have aa lot of adhesion. I’d plan on seeing an adhesion specialist at some point to fix this if you want to ever do this movements safely again. Not worth the risk otherwise.
Hunter Hayden
Posted at 03:59h, 04 FebruaryDr. Chris,
First off THANK YOU for all this content on dorsiflexion. I’ve got an interesting dorsiflexion issue and I’d be very appreciative to get your thoughts on it. I’m 29 years old and have been playing competitive basketball my entire life. I was recently playing in a pro-amateur game and did a spin move that caused a sharp pain in the left side of my lower back which my doctor has identified as sciatic nerve pain. But in the same moment I hurt my back, I lost about 80% of the strength when I dorsiflex my left foot and when I point my toe straight down I get a cramp below my calf muscle. This happened without feeling any pain in my left calf or achilles. It felt more like something when numb in there. I remember limping off the basketball court and it was like my leg was giving out. My left dorsiflex is about 1.75 inches and my right is about 2.25 inches. Based on your scale it seems my right leg is in big trouble too but so far I haven’t had any issues arise. My left side has had a few major and minor injuries.
Around age 15 I started having back spasms due to my right leg being longer than my left leg by about 5/8ths of an inch so I was recommended by a chiropractor to wear an orthotic with a lift in my left shoe. i sprained my left ankle a few times so I decided to have a cobbler put the lift on the outside of the shoe so my foot would go deeper into the shoe and that seemed to prevent ankle sprains. Then in 2016 I was playing basketball and made an awkward turn and fractured my left foot’s 5th metatarsal. After that healed I was back to playing basketball but I now had numbness in my left big toe that would get worse while playing basketball but would go away when I took my shoe off and rested.
So here I am now with 1.75 inch dorsiflex on my left and 2.25 inch on my right with numbness in my left big toe. I got a massage recently and the guy said that it felt like I have a layer of leather down my lower calf/achilles area and it’s a lot softer and normal on my right calf. I’ve been going to the gym to lift weights and do cardio on the machines. Should I stop doing things that work my calf muscle? Should I work with an ”adhesion specialist”? I haven’t heard of any of this until visiting your site today. My physical therapist through my insurance said I just need to massage it and do dorsiflex stretches and wiggle my big toe a lot but after about 4 months I’ve seen hardly any improvement.
I just want to be able to play basketball again. I hope that’s still possible. Where do you suggest I go from here?
Thank you,
Hunter
Dr. Chris
Posted at 16:46h, 04 FebruaryHello my friend – sorry for your struggles. It sounds like a lumbar disc issue with L4 nerve root involvement (big toe dermatomes) AND adhesion in the calf (flexor hallucis longus and likely the other deep tissues). I wouldn’t waste my time with anyone who isn’t an adhesion specialist. You’re throwing money away. Massage won’t improve that range. Yes, I’d stop strengthening becauses it’s not a muscular strength issue. It’s a neurological/adhesion weakness issue. Different problems require different solutions. Hope this is helpful.
Matt
Posted at 03:48h, 24 JuneThe evaluation of the “wall test” results must take into consideration height of the patient and proportions of their body in general. Obviously the taller the patient, the easier it is for him/her to reach the 5” of toe-to-wall distance. It’s just trigonometry. Your article does not address it in any way. I
Dr. Chris
Posted at 22:56h, 24 JuneYou’re 100% right. Practically speaking, we don’t find those types of details too be significant enough to address in the article – but they do need to be taken into account. Shorter people have max ranges of 4.5-5″ and taller people 7″ or so.
Remy
Posted at 04:19h, 04 December16 years old, 5’11 , 165 pounds, current dorsiflection is about 2,5″
Iv had somewhat slued feet for most of my life, its always felt natural for my feet to be in an inversion sprain position, it feels natural to just walk on the outer edge of my foot, almost asking for an ankle sprain. And i guess without really knowing it, iv never had very good dorsiflexion, i suspect its never gone over 3″, I guess i never understood why squating with heels down felt so unnatural, more so, impossible. and deep stances always seem to result in my legs squishing together, kinda makes me look like i have to pee if that makes sense. I guess its because my ankles are never dorsiflexed, because when i try to get my knee over my toes and then get in a stance my legs dont look as squished. but the real issue started last december (2019) when i had my first bad inversion sprain of my right ankle, i landed on this metal bar on the ground that caused a nasty roll, but i recovered within a few days, a couple months prior time i started getting serious about playing basketball, and joined my local 18u rec league, so when i sprained my ankle i was eager to make it back to practice, obviously not giving my ankle enough time to properly heal, but believe it or not i didnt sprain it again for a few weeks, until i stepped wrong on a protruding tree root on some uneven grass. Pretty much just as bad as the first sprain, from there on out it was a ton of minor instability rolls, up until late January 2020 when i had what i am pretty confident was a grade 3 sprain during practice coming up for a reverse layup, no idea how it even happened but it was some of the worst pain iv been in, i went to my family doctor for it and he grossly underestimated the injury and just kinda sent me back home, saying ill be cleared to play in 3 months, and i dont even need physical therapy, little did i know i wouldnt be able to walk for a month, and i felt like running was to dangerous to attempt for 4-5 months after the incident, finally the doctor had me refered for PT where i exercised 2-3 days a week. PT, which consistented of things like the wall stretch, some pilates machines, and some resistant band straining, never really seemed to help, and just from a few minutes of the wall stretch my entire ankle feels red and sore, as if i just sprained it again, – driving is another huge aggravator, just 20-30 minutes of driving can cause my ankle to cramp up and feel like its been sprained, sometimes ill have to use my left food at red lights etc because the pain is just too great.
So, i continued PT, i could have taken it more serious, no doubt, but regardless, my ankle just didn’t seem to be getting that much better, and id still just do light rolls of either ankle thoughtout a normal day (my left has never been sprained, but somehow has the same wall test results, and can feel very weak at times, obviously the right is much more suspectible to a quick roll) – usually these “rolls” dont even cause pain, because i catch myself before any tearing occurs, but it shows how unbelievably unstable my ankle is, these could happen 30 times a day, – I think all those years of causing inverting ankle, as a stretch or funky walk, has made me extra suseptable to the inversion
i cant express this enough, i physically cannot imagine rolling my ankle inwards, an eversion sprain, like i just cant see it happening, i cant preform it, my ankle just doesnt go that way? i dont get it, — as well as this my medial malleolus seems to be protruding quite a bit more than the average persons ankle, its like i have to balls attached to the inside of my feet, in a way that i when i look up photos of peoples ankles, i just dont notice it, and for me, its always been hard to even get my feet to touch perfectly together for things like martial arts, my medial malleolus would just smack into eachother and leave space, this was years before any sprains, and i also could not perform a regular squat with heal on ground, leading me to believe iv always had terrible ROM — after all that has happened, if i accidentally tap the tip of my medial malleolus to the pretty much anything, just bump it into a chair, table, or even just from bumping my two medial malleolus together, i experience some extreme pain, the type of pain that just feels like its sending a shock through my entire foot, it just makes you scream and fall onto your back as soon as possible, its so bad at this point that just thinking about it happening again can get me shaking – no doubt that my right medial malleolus is more swollen/protruding then my left due to the sprains, but my left medial malleolus seems to be overly protruding as well, like i said just slightly less than the right. i can link photos to everything from my medial malleolus, to the way my feet naturally rest on the inversion roll, im just not sure if ill recieve a response so ill add then after
Around August i finally was able to push for an MRI, and when the orthopedist saw me, all he had to say was basically, I have a noticable tear consistent with an inversion sprain, and i was told “the good news is you dont need surgery”, yet the original injury occured almost 7 months prior and iv been doing PT, so he just told me to continue on and report back
Around mid october I gained access to an air conditioned court near me, I hadnt sprained my ankle in a couple months and i was overconfident. I was there almost every day for a few weeks until in a full-court pickup game sprinting across the court, that naturally resting inversion position came into play, i landed on the outside portion of my foot and being that im sprinting as soon as i fully planted, i sprained it again, i was even wearing a lace up brace (i now have some newer more high quality ones) I could bear wait for a day or 2, and then was back to my instable ankle. this was about 3-4 weeks ago, so obviously im not playing basketball anytime soon, at this point, I just dont know what to do, the only thing that i enjoy is playing basketball, yet it would be completely idiotic to even attempt playing even with a brace for quite a while
Today I finally got back in with the Orthopedist, i pretty much told him a much less detailed version of this comment, he knows im not gaining the stability back and the tear is still there, and due to insurance we kind of need to get whatever needs to get done, done within 2020. – Hes referring me to someone who specializes in ankles more than him, and ill be seeing that new doctor monday, who will be basically be evalutating me for possible surgery, which is starting to look very likely at this point
i just hope i am not making a mistake, but assuming everything goes well, i could maybe have a much healthier right ankle by late january, and at that point my plan would be a complete rework and strenghening of my ankles, youd think at my age the ROM could surely improve? but i just pray im not incorrect, maybe theres some underlying structural/tight muscle issue along with the weak ankles and sprains limiting ROM as well, so im hoping that i can use the surgery as a way to undo my sprain in january, but i completely understand that my ankles were messed up to begin with and without some serious strengthening, ill just injure myself again.
at this point, im not sure how much righting a damn essay on my ankle can do, i hope my age adds some good optimism in this case. All i want to do is life is play basketball, and my dream is eventually playing in college. One of the things im most addicted to is jumping, dunking, and although i know even with a 40 inch verticle it due to my height it would never really add to my game to dunk occasionally, it is simply such a passion of mine that i do not want to give up. and I have a feeling these ankle injuries will never allow me to do what i want to do unless i want a very fine line to recovery
I guess i have to end this at some point, i feel like i have missed some of what i wanted to say, and then i obviously wrote about 5x too much– just want to throw this out there, my feet have always been sensitive, there was a point when i wore these size 14 shoes because any smaller meant my feet would cramp and feel red hot, i later realized the shoe was way to big for my foot and my real size was closer to 12, in length at least, a structured shoe at size 12 almost always caused great discomfort, – at first we hypothised i just have really wide feet, but i dont know as my foots greatest width doesnt seem to exceed 3 inches- I also have always experience a lot of pain from wearing ski boots, and i remember i physically could not wear snowboarding boots as within a minute or two i would be in so much pain i could hardly walk
last thing to keep in mind although i already mentioned it, my uninjured left ankle measures around 2.5″ and my injured right seems to measure in the same, so maybe the doriflextion is more affected by my gate then the injury itself –
if anyone manages to read all of this, thank you, i should have condensed this significantly
Dr. Chris
Posted at 21:45h, 04 DecemberRemy so sorry my friend. I get it. Football literally saved me from suicide in high school. SO I get it.
As far as regaining range of motion, I can’t say. I didn’t read anything in your essay about anyone telling you WHY you have restricted dorsiflexion. If we don’t have a diagnosis, I will assume it won’t get better.
If you’ve always walked “inverted”, you were likely born with “congenitally structurally different” ankles. A good ankle specialist who knows how to look at MRIs and all relevant angles should be able to help you.
Google “integrative diagnosis provider” and see if one of my colleagues are near you. Honestly, it’ll probably be the difference between you having horrible chronic ankle pain at 60 and being able to walk without issue.
Here fo ryou.
Kelley Hall
Posted at 19:41h, 12 SeptemberI took Cipro and Levaquin for 5 weeks for a Prostatitis in 2013, had odd heel pain even laying afterward. I went for a walk and it was like I was standing on my bones. Felt like real soft tissue damage. I went to a Doctor did an Xray said he saw bone spurs. Though I’ve been limping around and had weak ankles now for 8 years. I know that those antibiotics are notorious for soft tissue damage throughout the body… I’m constantly in pain on my left heel near the insertion of the achilles and the right acts up too when standing or using them. I tested my Dorsiflexion using your technique and I got 3 inches on the left and 4 on the right. I was rather athletic before this. Are there any suggestions you could have for me where to start or what would be safe? I missed my Podiatrist appointment due to time constraint and I didn’t feel they would help me much. Any and all help would be appreciated thank you. P.S. Those antibiotics are notorious for causing tendon necrosis and rupture…
Dr. Chris
Posted at 14:45h, 16 SeptemberHi Kelley, yeah they are. Can you find an adhesion removal doc? If not, best bet is a good PT or maybe shockwave therapy as well. You need to get that range better.
Joe Marri
Posted at 23:20h, 21 JulyI’ve been getting callouses on the inside of my big toe. Most of the providers tell me I need orthotics because I have a low arch, but the last two PTs I saw said my arch was ‘low but functional’. One day I just realized that I don’t let my foot dorsiflex it’s full range when I walk. I can relax and let it go much farther, but wasn’t sure if I’m supposed to use the full range of motion or not. Anyway I then realized I’m compensating for decreased motion by externally rotating my foot rolling the ankle in a little. I’m now pretty confident that this is what’s causing the callouses. I can also feel that, when I allow full dorsiflexion, the supporting muscles are not very strong. So after almost 3 years of treating “posterior tibialis” on the medial side, I now think I should be increasing dorsiflexion and strengthening posterior side. Anyway I’ll talk to a professional and confirm that, but I’ll definitely start working on range of motion! My number is around 4.5 but I know it doesn’t get anywhere close to that when I walk. Anyway, THANK YOU!!
Dr. Chris
Posted at 14:10h, 23 JulyGreat awareness. The question is, “If you have full dorsiflexion, why aren’t you using it?” Your body is compensating on purpose somewhere.
Maria Harrison
Posted at 06:12h, 10 JanuaryHello Dr.Chris
I was wondering if you knew anyone who does adhesion work near Huntsville Alabama(I’m willing to drive a couple hours out if needed). I was a rock climber and railed my left arch straight directly into a wall. The first month i didn’t think much of it I limped it off. Things started to feel really weird i couldn’t flatten my foot down and my arch and calf hurt. My arch and ankle and calf haven’t been the same ever since. I had two ankle mri’s and nothing was broken or torn and been in pt for over 6 months but my dorsiflexion and calve hasn’t improved much. At one point everything was so tight I couldn’t flex my toes up or down. I can’t squat without my lower ankle screaming because my foot is is so tight. My calf feels somewhat solidified together. I had harsh force directly on my arch and calf due to bracing myself with my leg as I swung towards a wall so it’s a weird injury not like I just rolled my ankle. Wondering if you know anyone in my area or I might consider even taking a trip to New Jersey.
Dr. Chris
Posted at 16:35h, 15 JanuaryHi Maria, there’s no one close. I suggest flyign to Precision Health Group in St Louis if you really want relief.
MikeQ
Posted at 18:57h, 21 JuneHi Dr. Chris,
I broke my ankle 4 months ago and received bad advice from doctors and my 1st physio.
I started seeing a better physio (6 weeks after cast was removed) who got me from 0 to 4.5/4.7 inches on the dorsiflexion test. However, I am now stuck at this point and have been for 4weeks or so. I keep reading that 5 inches is the minimum for sport (my healthy ankle is closer to 6 inches).
Can I do sports at this level and if not, are there any options (surgical or otherwise) to restore flexibility?
Would be so grateful for any advice!